You’ve undoubtedly heard about the Pfizer vaccine with a 95% effectiveness rate. It was all over the news. And now it’s been approved for emergency use authorization by the FDA and is being rolled out.
Later, after the press release from Pfizer, the study finally got published in the New England Journal of Medicine.
This is the journal that former editor Marcia Angell said, “It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of The New England Journal of Medicine.”
I looked through the study. I read the science. Despite what Forbes says, I like to do my own research. Because if we don’t, well, how damn easy do we make it for them to pull the wool over our eyes?
Here’s the study in question so that you can do the same:
Conflicts of Interest – Study Funding
Well, to be honest I didn’t start with the science itself, not at first. Here’s a tip! Instead, I looked at the conflicts. Why? Well, these seem to be a good shortcut to telling you what is really going on. In short, financial conflicts show a greater likelihood of bad science. By bad science I mean good for whoever is funding it and bad for the rest of us including the information ecology.
If this is new insight to you, here’s what you need to know on this topic. A 2003 systematic review published in the BMJ found, “Research sponsored by the drug industry was more likely to produce results favouring the product made by the company sponsoring the research than studies funded by other sources.”
A different systematic review from JAMA concluded, “Financial relationships among industry, scientific investigators, and academic institutions are widespread. Conflicts of interest arising from these ties can influence biomedical research in important ways.”
Reflecting on such, Sheldon Krimsky, in an article titled Science on Trial wrote, “Scientists typically believe that they are…objective of their inquiry, namely, the unfettered search for certifiable knowledge. While this is a widespread belief, it is not based on empirical evidence. Practicing scientists are least likely to know whether their conflicting financial interests affect the outcome of their research.”
This Pfizer COVID vaccine study? Let’s look at that little concluding paragraph.
“A two-dose regimen of BNT162b2 conferred 95% protection against Covid-19 in persons 16 years of age or older. Safety over a median of 2 months was similar to that of other viral vaccines. (Funded by BioNTech and Pfizer. ClinicalTrials.gov number, NCT04368728.)”
Maybe it is just me. But the most relevant piece of information is the ‘funded by’ statement.
This is my opinion, and I invite you to make your own, but this part leads me to discount the rest. I can’t trust it. And it’s not just the study funding itself.
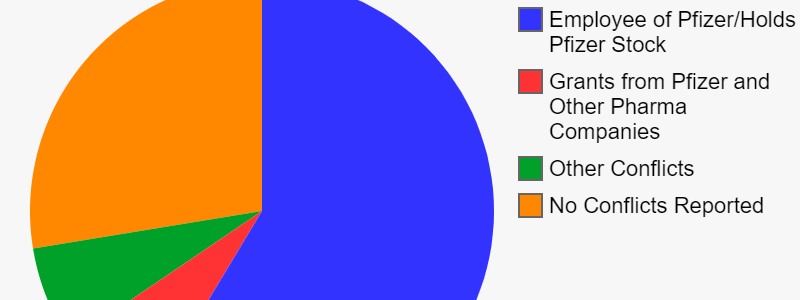
Conflicts of Interest – Author Funding
Not only that, but I looked at the disclosure forms for all the many authors on the study.
You can view the disclosure forms yourself here.
There are 29 authors on this paper. Of these:
- 16 are paid employees of Pfizer
- 1 is a former employee of Pfizer
- 15 hold stock in Pfizer
- 2 have received research grants from Pfizer
- 1 received fees as part of being a sub-investigator for the site in Argentina
- 1 received resources to their University where they worked during the trial
- 3 report personal fees or grants from other pharmaceutical companies
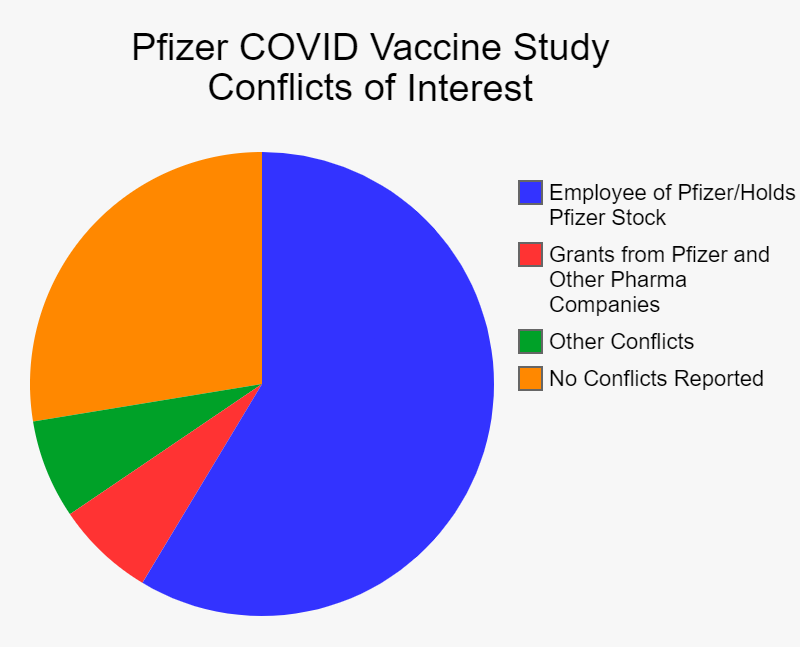
Over half the people stand to gain directly as a positive result of this trial. Do you think their might be bonuses, promotions or other incentives when the Pfizer stock shoots upwards and revenues break records?
Conflicts of Interest – Hidden Away?
Please keep in mind this is what was freely disclosed. Unfortunately, we sometimes see stuff hidden away. (Dr. Jose Baselga is a good example of this if it’s new to you.)
With a quick search I found that Edson Duarte Moreira, one of the people who said there was no relevant conflicts in this study, is by no means clean of past conflicts.
In a 2014 paper on HPV, he listed “received grants through his institution for conducting HPV vaccine trials, consulting fees, support for travel, fees for board membership, and fees for lectures from Merck.”
Merck is one of two companies that makes the HPV vaccine. Turns out he’s author on a bunch of HPV vaccine trials.
A 2013 paper says he “has received grant support through his institution from Sanofi-Aventis, Merck, Pfizer and Novartis, and was compensated by Sanofi-Aventis, Merck and Pfizer for serving at Scientific Advisory Committee.”
So, he had been paid directly by Pfizer in the past. Just not in the 3 years required to disclose.
Bottom line, he has shown a pattern of being paid directly by the company that stands to gain the most from positive research.
So I don’t trust the science from the get-go. But assuming I did, let’s look at the science, shall we?
PCR Testing Revisited
Since my previous article where I address PCR testing false positives, the WHO has come out (quietly) and admitted that there is a problem.
The WHO says, “the cut-off should be manually adjusted to ensure that specimens with high Ct values are not incorrectly assigned SARS-CoV-2 detected due to background noise.”
That’s geek-speak for saying that many COVID cases are not real cases. Just background noise.
So at this point we have Fauci saying it’s a problem. We have the New York Times saying it’s a problem. We have the WHO saying it’s a problem.
Mainsteam and credentialed sources…and still people won’t be convinced. Frustrating, I know.
I bring this up because this Pfizer vaccine trial relies on what? We have to dig into the 376-page protocol of the trial to find this.
“Efficacy will be assessed throughout a participant’s involvement in the study through surveillance for potential cases of COVID-19. If, at any time, a participant develops acute respiratory illness, for the purposes of the study he or she will be considered to potentially have COVID-19 illness. In this circumstance…assessments should be conducted…The assessments will include a nasal (midturbinate) swab, which will be tested at a central laboratory using a reverse transcription-polymerase chain reaction (RT-PCR) test.” (pg 51)
Note that antigen testing was also used, which is fraught with its own problems.
So I searched this document for everywhere using the terms “PCR”, “cycle”, “count”, “ct”, “threshold”. While there are many instances of these words, none of them have to do with what the PCT test Ct value was set too.
They make mention of the FDA’s emergency use authorization regarding the PCR test. The FDA’s document recommends a setting of 40 cycles. (found on page 35)
Most everyone else is saying that anything above 35 is meaningless. Many are saying 30 or 25 is far better.
So, in the end, this trial is unscientific because it relies on a faulty test.
How to Lie with Statistics
Well, maybe not lie, but certainly spin!
Let’s assume we can discount all the conflicts, even though we shouldn’t. Let’s assume the test was valid, even though as we’ve seen it is not. Let’s get to the actual study data.
The study had 37,706 people received both doses of injections. 18,556 got the vaccine. 18,530 received placebo injections.
The cases only counted if the onset was at least 7 days after the second dose. Had the onset been anytime, then lots of vaccinated people would have been tested because many of the side effects of the vaccine are an awfully similar to the symptoms of COVID. That’s a very specific window of time supposedly because they have to give the vaccine time to build the spike proteins to ward off the invader.
In this time frame, 8 people who got the vaccine tested positive for COVID. 162 people who got the placebo tested positive for COVID.
In this time frame, 1 person who got the vaccine had a severe case of COVID. Nine people who got the placebo had a severe case of COVID.
From this they do some statistical analysis to arrive at that 95% efficacy mark.
“Vaccine efficacy was estimated by 100×(1−IRR), where IRR is the calculated ratio of confirmed cases of Covid-19 illness per 1000 person-years of follow-up in the active vaccine group to the corresponding illness rate in the placebo group. The 95.0% credible interval for vaccine efficacy and the probability of vaccine efficacy greater than 30% were calculated with the use of a Bayesian beta-binomial model. The final analysis uses a success boundary of 98.6% for probability of vaccine efficacy greater than 30% to compensate for the interim analysis and to control the overall type 1 error rate at 2.5%.”
I’ll be honest. Without reading up on it, that’s above my statistical skills. But something I do know is that this shows something call relative risk. Let’s look at absolute risk instead. Much easier statistics.
According to these numbers, your chance of catching symptomatic COVID:
- 170/37706= 0.451% overall
- 162/18530 = 0.874% without a vaccine
- 8/18556 = 0.043% with a vaccine
Keep in mind this is any symptoms at all, like a cough or fever. We’ll come back to that subject later. So that vaccine is lowering the chance you get any COVID symptoms over .8% in absolute terms.
And your chance of a severe case of COVID which includes “respiratory failure; evidence of shock; significant acute renal, hepatic, or neurologic dysfunction; admission to an intensive care unit”.
- 10/37706 = 0.027% overall
- 9/18530 = 0.049% without a vaccine
- 1/18556 = 0.005% with a vaccine
Here we see a lowering of 0.044% in absolute terms. That is far, far less than 0.1%.
Six people died in this study (“Two BNT162b2 recipients died (one from arteriosclerosis, one from cardiac arrest), as did four placebo recipients (two from unknown causes, one from hemorrhagic stroke, and one from myocardial infarction). No deaths were considered by the investigators to be related to the vaccine or placebo.”)
But this is key. No one died of COVID in this study.
So according to it, your chances of dying are 0% with or without the vaccine.
(The cynical joke is if it hadn’t been in this study, there’s a good chance some or all of those deaths would be COVID deaths!)
A Different Conclusion
Now, I don’t know about you, but looking at those stats my first takeaway is not that the vaccine is 95% effective…
…but that COVID is not worth worrying about!
Oh how I wish the headlines read, “Pfizer vaccine study a waste of time and money as COVID not as harmful as thought”
If you look at the stats, the vaccine study itself is showing you this!
Just to be clear, I’m not denying that it is virus isn’t hurting some people. Nor that certain high risk groups might want to take some precautions.
Instead, I’m saying that the worldwide response, lockdowns, masks, social distancing, etc. is unwarranted…if health is the actual concern.
And most certainly that mandating this vaccine is ludicrous.
But, alas, this has nothing to do with health.
And don’t forget that this study was never intended to show that it would stop or slow the spread of SAR CoV-2. Yet, somehow that is what people will magically believe. Because, you know, science.
Then you have to factor in the next part…
Pfizer Vaccine Side Effects
The adverse event reporting in this study only extended 14 weeks after the second dose.
More so than acute symptoms, I’m more worried about longer term stuff. Autoimmunity for instance can take years to develop. Same with cancer. Then there’s the whole infertility thing which certainly isn’t caught in this short time frame.
Hopefully there is none of these. But you can’t say scientifically that they aren’t. We just don’t know is the only valid scientific opinion. After all, this mRNA vaccine is brand new technology never before used in human beings.
And the fact is that they’re crossing over the placebo patients into the vaccine group (because its so effective it would be unethical to deny them the real vaccine so they say). This means we will not actually have useful long-term safety data from this.
Therefore, the two year safety follow-up won’t really show us any long term effects.
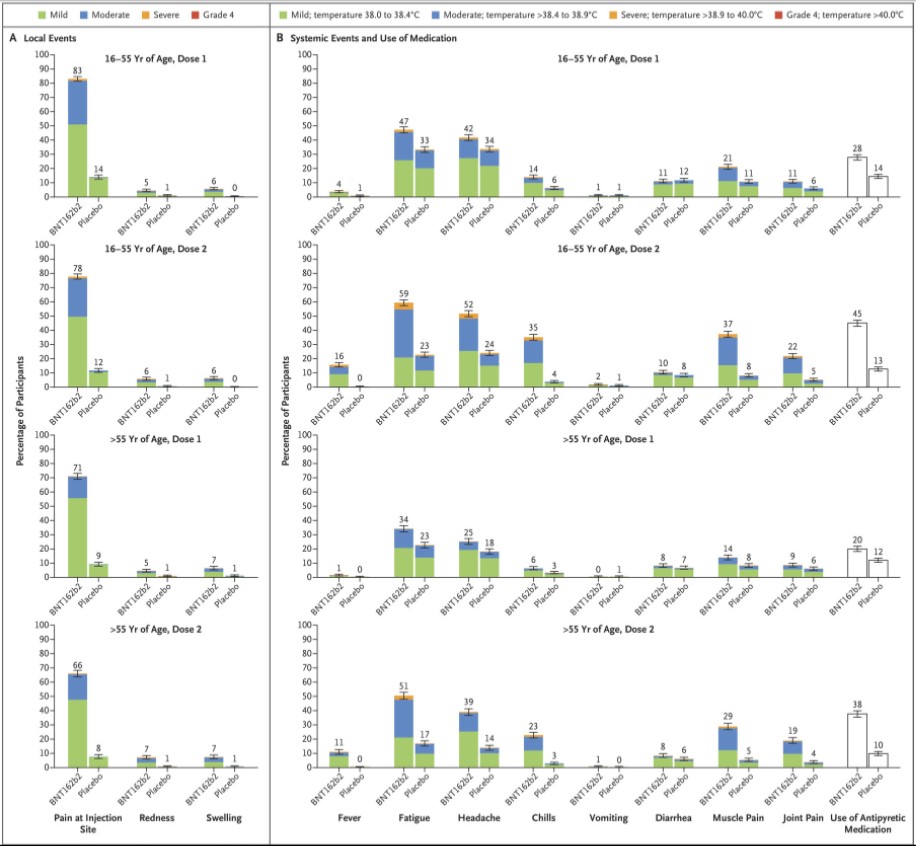
Still let’s look at the short term risks. Here’s some of what the study lists as for side effects:
- “Severe systemic events were reported in less than 2% of vaccine recipients after either dose, except for fatigue (in 3.8%) and headache (in 2.0%) after the second dose.”
- “Fever (temperature, ≥38°C) was reported after the second dose by 16% of younger vaccine recipients and by 11% of older recipients.”
- “More BNT162b2 recipients than placebo recipients reported any adverse event (27% and 12%, respectively) or a related adverse event (21% and 5%).”
Just compare these percentage numbers to the amounts who got COVID, even the unvaccinated group, above.
Here’s another conclusion or headline we didn’t see. “Pfizer Study Finds Vaccine Causes 2-5X as Many Symptoms as COVID.”
I’ve said it before, and I’ll say it again. I’d rather take my chances with the coronavirus then with this vaccine.
The short-term side effects show much more likelihood of symptoms than COVID. They seem worse. And we aren’t sure about the long-term effects yet.
Current Side Effects Tracking
Just to expound this point further, here’s a slideshow from the CDC showing the surveillance of the COVID vaccine rollout. (Note that this likely includes the Moderna vaccine as well as Pfizer vaccine. We did not cover the former here.)
On December 18th 112,807 people had received the first dose.
Of these 3,150 have health impact events which are defined as “unable to perform normal daily activities, unable to work, required care from doctor or health care professional”.
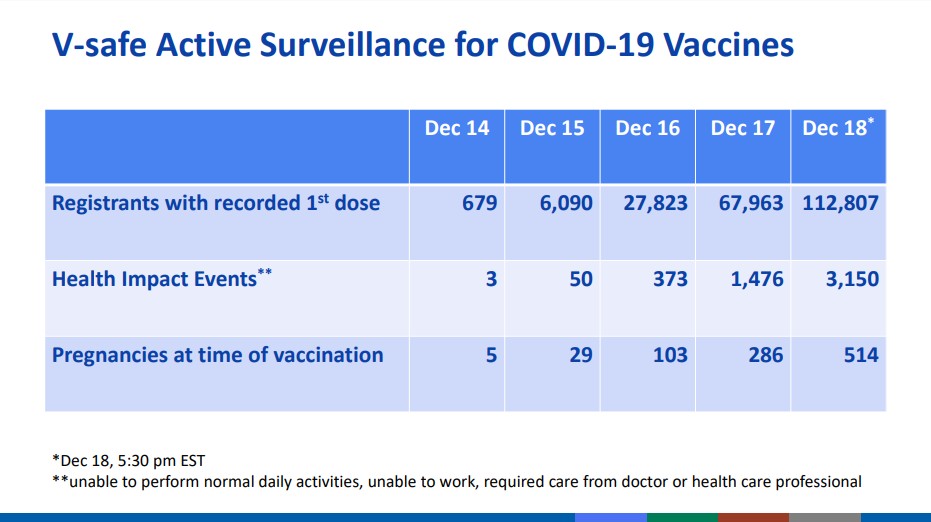
3150/112807 = 2.792%
Please compare that percentage number with the 0.746% of any COVID symptoms without a vaccine in this study, let alone the 0.041% of severe COVID.
Note that unable to perform normal daily activities is worse than the any COVID symptom group, though not necessarily as bad as the severe COVID group.
Hopefully, that is a one-time adverse event that the people bounce back from. What is worrisome is to think that with that, there is likely some systematic longer-term consequences.
Just some more extremist, terrorist, anti-science, anti-vaxxer, Russian misinformation for your to think about for yourself.
Love it? Hate it? Questions? Other resources to look at? Leave them in the comments below…
It’s interesting that no one is mentioning that “operation warp speed” bypassed the animal testing phase. In the previous trials to create a Corona virus vaccine, all seemed to be going well til the animals (ferrets) were exposed to a wild form of the virus. Then their immune systems kicked into overdrive and they died horrible deaths. I guess the test animals this time are us.
Hey David, do you have any reference to those studies? I’ve been hearing that from several sources, but have yet to see the original reports
These studies cover the subject though there are certainly other sources:
https://www.nature.com/articles/s41577-020-00434-6
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7142689/
That’s old news, not that it’s not important. Even Dr. Peter Hotez was talking about it. Definitely a possible issue, though supposedly some of these people were exposed if you could believe the numbers.
Interesting. So what is the long term goal? What does life look a year from now?
Stay tuned, my next article is 2021 predictions.
Great information and analysis Logan! Ok, so I have been trying to get to the bottom of the Ct topic. I have called around to multiple labs, and none use less than 40 Ct so far.
So I ask a few more questions to the lab:
1) Where is it in writing that your lab/test use “40 Ct”? (I am told by the lab tech “that is proprietary information, and cannot be released. But our testing/equipment is CLIA certified.”) So that was not helpful. What does CLIA have to do with the Ct? I guess the lab will just “defer” to CLIA to explain to use why they use 40 Ct?
2) “Who” (haha) authorized that Ct value? I have not been provided any answer to that yet. However, now that I see in your post that the FDA Emergency Authorization for PCR testing recommended using 40 Ct, that makes me far less confident anyone will take responsibility.
Where exactly did the FDA pull this “40” value from? Now that the WHO said the PCR is faulty, did the FDA or WHO explain why they used “40” to begin with?
Just saw these video which mentions Florida is now making labs report the numbers. That will be interesting to watch play out.
https://theconsciousresistance.com/the-pcr-deception/
I also came across this study that talks about using PCR with influenza and viral load. The interesting thing here is they are using “Ct value was categorized into three groups (low Ct, ≤ 20; intermediate Ct, > 20–30; and high Ct, > 30)”. https://link.springer.com/article/10.1007/s10096-019-03514-1
The cT value is the cycle at which the value surpasses a certain treshold (and this treshold can be adjusted). The number 40 that you use refers to the amount of cycles of the PCR program and has no effect whatsoever on the outcome. 40 is just fine, because everything there is to see has already happened before cycle 40.
I have not seen the PCR tests they use for COVID, but I perform a lot of PCRs and qPCRs myself.
I get from this that the PCR they use is a quantitative PCR that is supposed to provide a yes/no answer based on the cT (cT low enough = positive, cT too high or just none existent = negative.)
There is either amplification or there isn’t. For the most part this is very simple, but for higher cT’s this becomes a little more tricky. The higher the cT, the less material (virus) was present before amplification. It is difficult to name a cutoff, because minuscule contaminations in the water might still produce a high cT value. Normally a water sample is taken along to make sure the water isn’t contaminated. Roughly up to cT 35 could count as positive. Ideally qPCRs are designed to produce cT’s under 30, since quantification is more accurate then, but depending on the input material and the expression of the target, this might not be possible. In general qPCR is an extremely sensitive and extremely accurate technique. The only problem might be to judge the high cT cases, which should be rare if the procedure was designed well. I would have to see every step in the protocol and also the output of the qPCR machine to judge which cases are positive. Your water should be a flat line that never crosses the treshold, but it can certainly happen that it reaches a cT of 36 or something. (This corresponds to an extremely low amount of starting material, maybe just 1). Clearly all samples with a cT of 36 or higher shouldn’t be considered positive then. A ct of 40 is easy, no way that is positive.
Thanks for sharing your opinions from someone that actually uses these things. The FDA document linked to in this post, or maybe it was in the previous post, might have more the the steps broken down in there. I wouldn’t be surprised if it’s not clear at all though.
You’re not the only one unconvinced by this rather improvised drug.
Here’s an interesting read, the legal petition by a couple of experienced medic/researchers to the European Medicines Agency (regulator in the EU) specifically concerned about the Antibody Dependent Enhancement issue mentioned above.
https://sarahwestall.com/wp-content/uploads/2020/10/Wodarg_Yeadon_EMA_Petition_Pfizer_Trial_FINAL_01DEC2020_EN_unsigned_with_Exhibits1.pdf
Yeah I saw that out there. People want to listen to Pfizer but won’t believe the whistleblowers that come out of Pfizer at all. That seems odd to me.
Thanks for breaking it down so clearly. I had caught the highlight data on the rates vs placebo and came to the same conclusion to take on whatever risk there might be facing the disease vs the unknown of the faces.
I’m wondering if the flu I got in Jan 2017 gave me antibodies to it as that was the worst illness I’d ever had.
The unknown of infertility and pathogenic priming are the two big ones I’m not interested in risking for my kids.
Plus, I think there’s a case to be made that vaxes increase the likelihood of Alzheimer’s and likely calcifies our pineal gland, diminishing our intuition and connection to the universe in the process.
Jeez.thank you so much for this breakdown.